RECAP: Relational Communication in Dementia Care
RECAP: Relational Communication in Dementia Care
A practical, rights-based framework to support identity, autonomy and inclusion for older adults from culturally and linguistically diverse (CALD) backgrounds
Relational communication in dementia care: Supporting identity, autonomy and inclusion for culturally and linguistically diverse (CALD) older adults
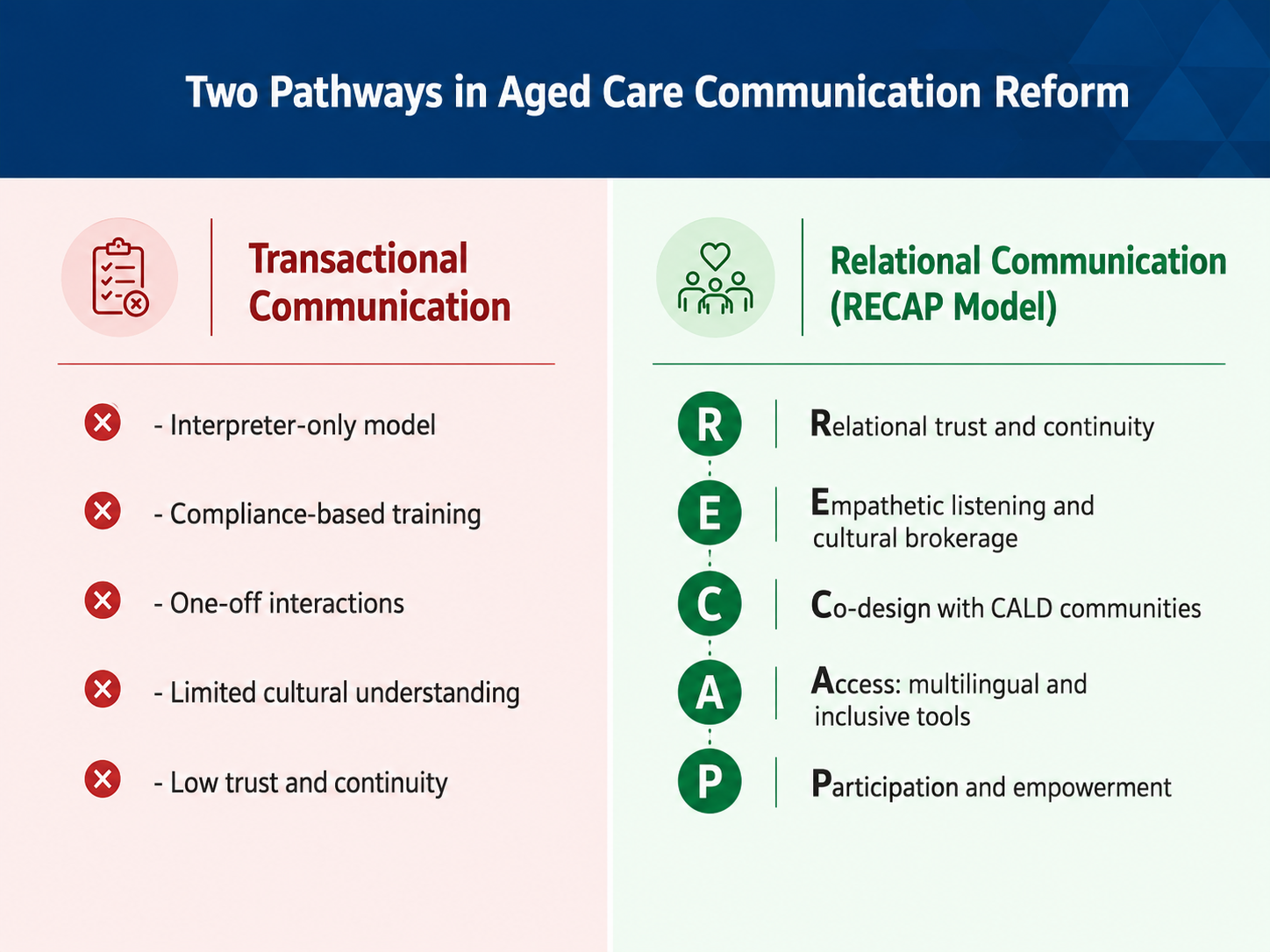
Communication in dementia care is often framed as a technical challenge – solved through interpreter access or translated materials. Yet for older adults from ethnically diverse communities, language barriers are deeply relational, affecting trust, autonomy, and emotional wellbeing. This presentation introduces a relational model of communication that reframes communication difficulties, language reversion and care navigation as identity-affirming processes requiring continuity, empathy, and cultural understanding.
Drawing on a qualitative systematic review of 51 international studies and early findings from a PhD study on older Polish Australians living with dementia, the presentation explores how evolving care needs intersect with ageing in place. It highlights the role of family and chosen support networks in bridging communication gaps and co-creating culturally safe care environments. The RECAP framework (Relationships, Empathy, and Cultural understanding through Access and Participation) is proposed as a practical model for embedding relational communication into dementia care.
The presentation will share lived experience insights, policy implications, and practice recommendations for workforce development, service design, and community engagement. It contributes to the broader conversation on personhood, dignity, and inclusion in dementia care – moving beyond compliance to connection.
Downloadable Handout
This handout is an accompanying document for the International Dementia Conference 2026, please click the link below to access/download the handout:
Communication is for everyone. CALD makes the system more fragile
Communication matters for everyone. In dementia care efficient communication shapes trust, autonomy, consent, safety, belonging and quality of life. CALD contexts function as a quality “stress test”: when services reliably support diverse languages and cultural frames (including in-language support and interpreter engagement), communication pathways become clearer, safer, and more inclusive for everyone. When we get communication right for people living with dementia across languages and cultures, we improve quality, dignity and inclusion for everyone, not only for those who need in-language support.
In CALD contexts (Culturally and Linguistically Diverse communities in Australia), the system fragility is caused by practice gaps around: language mismatch, interpreter-mediated encounters, different norms around consent and decision-making, stigma, and reliance on informal networks to navigate services.
We know from caregiver education research that what changes outcomes is often not more effort, but a better framework. When carers shift from controlling tasks to building connection, cooperation improves and distress can reduce. In summary, frameworks change behaviour, not just knowledge.
RECAP offers a practical way to meet the ‘stress test’: turning language access into relational safety, autonomy and inclusion.
Key sector term: in-language support: a whole-of-pathway approach that enables understanding and participation communicating in the person’s preferred language. In-language support requires: bilingual capacity and interpreter engagement and providing in-language information* and culturally grounded navigation* and community-connected support*).
* in a co-designed person-tailored user-friendly format
Rights-based anchor: Communication is not a “nice-to-have
Australia’s Aged Care Act 2024 (Cth) establishes a Statement of Rights (Part 3), including rights linked to autonomy, privacy, connection to significant persons, and person-centred communication.
Government guidance on the new rights-based Act explicitly links quality care to respecting identity and communicating in preferred language (including interpreters where needed).
Policy alignment: The National Dementia Action Plan 2024–2034 centres equity, human rights, inclusion, workforce capability and carer support – creating a strong policy context for operationalising relational communication.
What RECAP is (take-home)
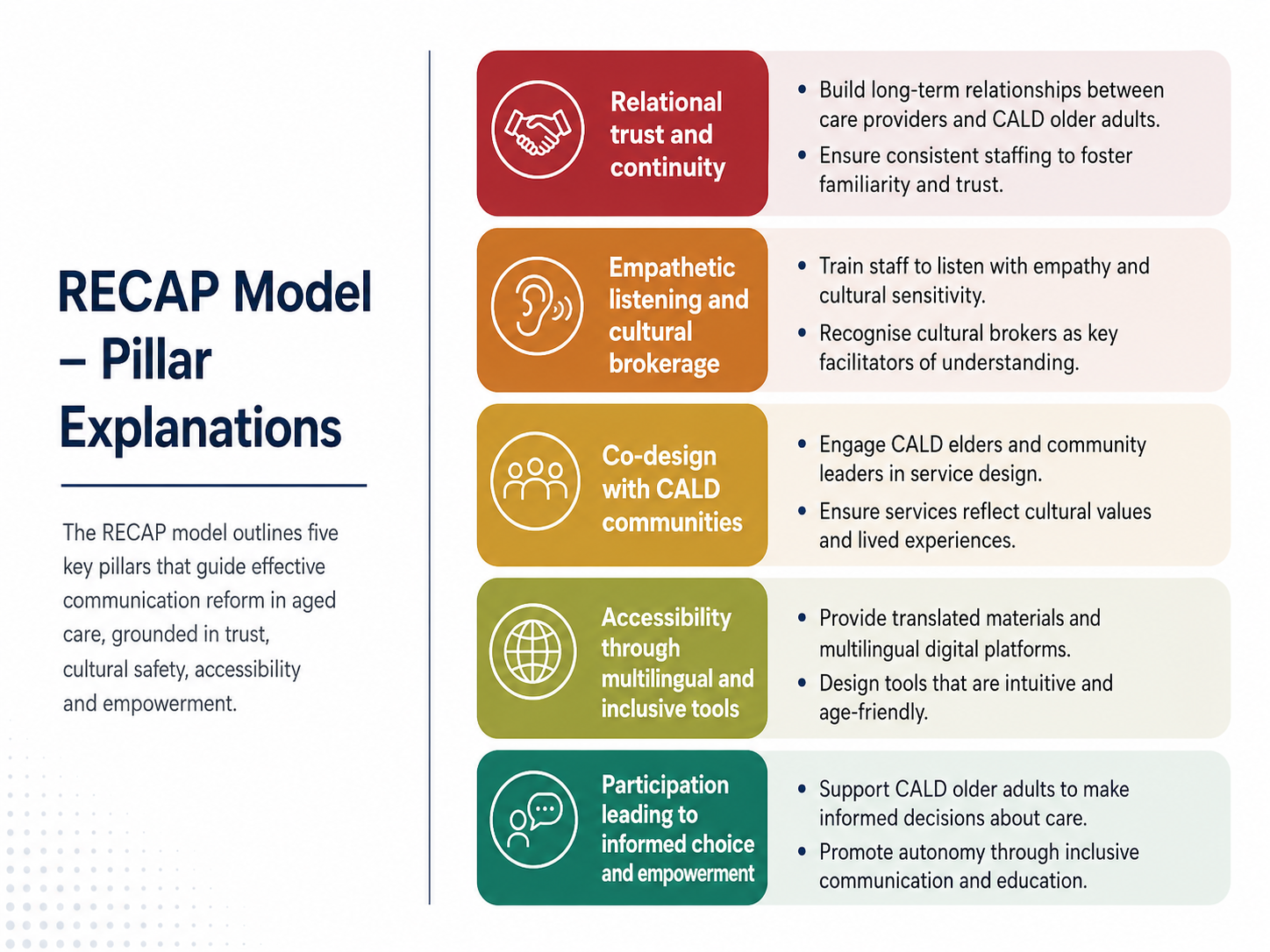
RECAP = Relationships, Empathy, Cultural understanding through Access and Participation.
Take-home line: Interpreter access is necessary, but not sufficient. RECAP is how we turn access into dignity, autonomy and inclusion.
There are well-established relational frameworks that also start from understanding the person’s lived experience. One example is Teepa Snow’s GEMS® State Model, which encourages care partners to focus on retained abilities and respond to the person’s current brain state rather than trying to force a preferred outcome.
RECAP unpacked (R, E, C)
R - Relationships (continuity beats speed)
Aim: Build a trusted relational base so communication doesn’t collapse under stress, progression, or language shifts.
In practice (what you can do):
- Prioritise continuity (known staff / trusted contact).
- Use a relational handover (what matters, what works, what escalates, what calms).
- Treat communication as a care intervention, not a task add-on.
E - Empathy (listen beyond words - including body language)
Aim: Hear meaning, emotion and needs even when words reduce or change.
In practice:
- Slow down; validate; reflect meaning back.
- Flag: Actively attend to body language (gaze, posture, gesture, pacing, tension, withdrawal, agitation), especially when language is limited or interpreter-mediated.
- When distress escalates, assume a communication need before assuming “behaviour”.
Bridge sentence:
“Help me understand what feels hard right now.”
C - Cultural understanding (meaning, not stereotypes)
Aim: Understand identity continuity: migration story, values, family roles, stigma, norms of respect, and what “good care” means in that person’s world.
In practice:
- Ask about life story and what “matters most”.
- Recognise cultural norms shaping consent, privacy, who speaks, and how distress is shown.
- Use cultural understanding to adapt care, not label people.
RECAP unpacked (A, P)
A - Access (normalise interpreter engaged + in-language support)
Aim: Ensure language support is usable, timely and embedded—not merely “available”.
In practice:
- Record preferred language early, visibly, and re-check over time.
- Normalise interpreter engaged as a routine pathway (not a special request).
- Track uptake, note refusal, and repeat the offer later (needs/ preferences change).
- Brief and debrief with interpreters; avoid shifting interpreter labour onto families.
TIS National (Australia) – two useful links:
- Immigration/ Home Affairs TIS page:
https://immi.homeaffairs.gov.au/settlement-services-subsite/Pages/tis-national.aspx - Health.gov.au contact page for TIS National:
https://www.health.gov.au/contacts/translating-and-interpreting-service-tis-national
P - Participation (make needs visible early)
Aim: Services can only address communication needs if the system makes them visible and legitimate.
In practice:
- Include the person with dementia in decisions in the way that works for them (supported decision-making).
- Build feedback loops and co-design with CALD communities (participation beyond tokenism).
Operationalising RECAP: indicators that “force” inclusion
NDAP progress is tracked through indicators. This logic can be applied to relational communication to make it non-optional.
Starter indicator set (adapt locally):
Starter indicator set (adapt locally):
- Preferred language recorded and reviewed.
- Professional interpreter engaged: uptake tracked; refusal noted; repeat offer later.
- Continuity metric (trusted contact/ relational handover).
- Carer consent documented and revisited.
- Evidence of CALD participation/ co-design feedback loops.
Quick-start RECAP (2 minutes):
Quick-start RECAP (2 minutes):
- R: “Who do you trust most in your care team?”
- E: “What feels hard today? What would help?” AND observe body language.
- C: “What should I understand about what matters to you?”
- A: Confirm preferred language AND interpreter engaged plan; repeat offers.
- P: “Who do you want involved in decisions? And how?”
In-language support across the pathway
In-language support across the dementia care pathway (Use this as a template)
A pathway view makes in-language support predictable and resourced, rather than crisis-driven.
Diagnosis & assessment
- Preferred language check and interpreter engaged plan; dementia-aware briefing/ debriefing.
Post-diagnosis support and navigation
- In-language information; culturally safe explanation; link to community supports.
Care planning
- Include chosen supports; document consent and boundaries; revisit over time.
Coordination and ongoing care
- Continuity and relational handover; interpreter engaged when needed; repeat language preference checks.
Review and changes (including crisis)
- Repeat interpreter engagement offer (uptake/ refusal may change); capture feedback loops.
Best Practice
Evidence example (best practice): MINDSET
The MINDSET Study (NARI) describes co-design, trial and national implementation of dementia-specific interpreter training, including dementia knowledge and briefing/debriefing.
A peer-reviewed implementation paper reports national rollout of interpreter training for dementia assessments.
(Disclosure: Presenter references MINDSET as an external best-practice example, not as a project member.)
Carers, Bridge People, indicators and references
Carers and consent: Stop assuming, start asking
Rights-based aged care emphasises autonomy, person-centred communication and connection to significant persons. This requires explicit, ongoing consent and support planning with carers.
Use these prompts in care planning:
- “Do you consent to being involved in communication support? In what way?”
- “What boundaries should we protect (privacy, emotional load, time)?”
- “What would most help you in your caregiving role?”
- “What is your #1 priority right now?”
- “Would engaging a professional interpreter reduce pressure or risk?”
The intergenerational language gap (repeat the question over time)
Preferences and capacity shift across dementia progression; repeat these questions in reviews, not only at intake.
- “What language do you feel safest in when tired, stressed or unwell?”
- “Who communicates best with you in that language?”
Best Practice
“Bridge People”: Recognise the real connectors (reference included)
“Bridge People” are trusted bilingual/ bicultural supporters who help older migrants navigate services; attributes include bilinguality, biculturality, multifunctionality and accessibility.
Reference: Liu X, Cook G, Cattan M. Support networks for Chinese older immigrants accessing English health and social care services: the concept of Bridge People. Health & Social Care in the Community. 2017;25(2):667–677. doi:10.1111/hsc.12357.
Bibliography
Key References
- Australian Government Department of Health and Aged Care. (2024, December 5). National Dementia Action Plan 2024–2034. https://www.health.gov.au/resources/publications/national-dementia-action-plan-2024-2034
- Chudecka, A., Xiao, L. D., & Muller, A. (2023). The experiences of older migrants with language barriers in accessing and utilising care services: A qualitative systematic review (PROSPERO registration CRD42023491183). International Prospective Register of Systematic Reviews (PROSPERO), Centre for Reviews and Dissemination, University of York. Available from https://www.crd.york.ac.uk/PROSPERO/view/CRD42023491183
- Chudecka, A., Xiao, L. D., & Muller, A. (n.d.). Older Migrants, Language and Access to Care: A Qualitative Systematic Review. [Manuscript under review].
- Feurich V. 6 GEMS® You Need to Know For A Positive Approach to Dementia Care. Positive Approach to Care (TeepaSnow.com). 10 Jul 2019. [linkedin.com]
- National Ageing Research Institute. (2024, June 6). MINDSET Study: Improving interpreting for dementia assessments. https://www.nari.net.au/the-mindset-study
- National Ageing Research Institute. (2025, February 12). Online interpreter training improves dementia detection (Media release). https://www.nari.net.au/news/online-interpreter-training-improves-dementia-detection
- Liu, X., Cook, G., & Cattan, M. (2017). Support networks for Chinese older immigrants accessing English health and social care services: the concept of Bridge People. Health & Social Care in the Community, 25(2), 667–677. https://doi.org/10.1111/hsc.12357
- Positive Approach to Care. Seeing the GEMS Workbook, includes bonus videos. [teepasnow.com]
- Rubio OC, Husser EK, Wright R, Berish D, Whitaker J, Boltz M, Fick D. “I Must Be the One to Change; He’s Doing the Best He Can”: Care Partner Evaluation Results from a Four-Part, In-Person, Dementia Community Education Program. Int J Environ Res Public Health. 2025;22(2):295. doi:10.3390/ijerph22020295. [au-prod.as…rosoft.com]
- Translating and Interpreting Service (TIS National). Department of Home Affairs. (n.d.). About the service. https://immi.homeaffairs.gov.au/settlement-services-subsite/Pages/tis-national.aspx
Recommended/Further Reading
- Australian Government Department of Health, Disability and Ageing. (2025, December 22). National Dementia Action Plan overview. https://www.health.gov.au/resources/publications/national-dementia-action-plan-overview
- Australian Government Department of Health, Disability and Ageing. (2026, February). National Dementia Action Plan collective priority framework 2025–2027. https://www.health.gov.au/sites/default/files/2026-02/collective-priority-framework-2025-2027.pdf
- Australian Government Department of Health, Disability and Ageing. (2024). Summary of National Dementia Action Plan 2024–2034. https://www.health.gov.au/resources/publications/summary-of-national-dementia-action-plan-2024-2034
- Brijnath, B., Cavuoto, M., Markusevska, S., & Clarke, N. (2025, January 31). Improving interpreting for dementia assessments: The MINDSET study—National implementation (Stage 3) final report. https://www.rmit.edu.au/content/dam/rmit/au/en/about/schools-colleges/guss/social-equity-research-centre/projects/mindset-implementation-final-report.pdf
- National Accreditation Authority for Translators and Interpreters (NAATI). (2023, January 16). Free dementia training for interpreters: MINDSET project. https://www.naati.com.au/news/mindset-dementia-interpreter-training-trial/
- Translating and Interpreting Service (TIS National), Department of Home Affairs. (n.d.). About us. https://www.tisnational.gov.au/en/Who/About-us
Key References (for teams/policy briefs)
Chudecka, A. (2026). RECAP: Relational communication in dementia care. Supporting identity, autonomy and inclusion for CALD older adults. Handout, International Dementia Conference (IDC), Sydney, Australia.

